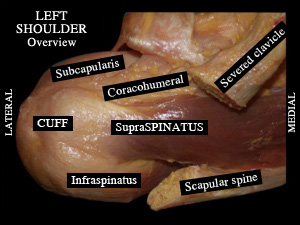
The rotator cuff is a group of four tendons (subscapularis in front, supraspinatus on top, infraspinatus and teres minor at the back) in which must be counted the long biceps tendon that slides forward through a sheath located between two tendons. They converge from muscles connecting the scapula (shoulder blade) to the top part of the humerus where they are solidly fixed. Their role is to enable arm rotations and ensure arm mobilization above the horizontal plane.
Before surgery :
The cuff tendons will tend to wear away over time or after excessive efforts required from the shoulder (repetitive gestures, working with the arm overhead).
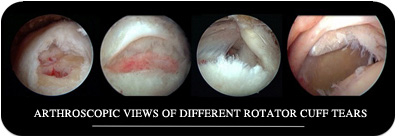
The pathology evolves gradually toward a detachment of the bone tendons from the head of the humerus, this is then known as rotator cuff tear or (« hole though the rotator cuff tendon »). When tendons suffer but remain attached to the bone, the pathology is then known as tendinopathy or rotator cuff « tendonitis ».
Pain is frequent, more or less intense or permanent according to each case, and occurs more often than not during the night. In most cases the shoulder voluntary movements are not limited, even in presence of a cuff tear although loss of strength can usually be observed when raising arm overhead.
After thorough clinical examination and reading of the simple X-rays of the shoulder, which is done systematically, the physician will be able to require further examination to precisely assess the condition of the cuff tendons by means of: echography, artro-MRI, arthroscan (injection of a product into the joint for the last two ones) or MRI.
The first stage of the treatment involves specific physical therapy exercises suited to the cuff disorder, possibly associated with one or two infiltrations into the shoulder.
For the surgeon to opt with his patient for a surgery procedure on his shoulder, several conditions are required: both the failure of well-conducted medical treatment over a few months and a complete rotator cuff imaging with a flexible shoulder.
In presence of a young, active and sportive patient suffering from a traumatic tear, the surgery indication will be taken very rapidly.
During surgery :
Arthroscopic surgery is performed in this procedure. (Arthroscopy is a technique using a small camera inserted through a small incision into the shoulder). The duration is variable according to the number and to the importance of the movements performed in the procedure; (from 10 to over 2 hours)
The surgical treatment will be suited to the pain described by the patient, to the clinical examinations and the rotator cuff condition.
If there is a rotator cuff tear, the treatment will depend on the size of the tear (number of tendons torn, tendon retraction at the extremities), on the quality of the cuff muscles and on the patient (age, general condition, motivation, sports or leisure activities .). Repair is not always systematic and remains sometimes impossible in case of massive tears.
The repair aims at re-attaching tendons to the head of the humerus where they are normally inserted, with the help of suture anchors drilled into the bone. Suture threads pass through these anchors and enable to bring and flatten the tendon back over the bone to facilitate healing.
Rupture of the rotator cuff – Arthroscopic Repair
After surgery :
After surgery the shoulder is immobilized with the help of a comfortable splint maintaining the arm along the body with the elbow folded (arm sling and shoulder brace). When an important rotator cuff tendon repair has been performed, it may be necessary to immobilize the shoulder with a sling by keeping the arm off the thorax.
The immobilization duration depends on the type of the procedure movements performed under arthroscopy. (1 to 6 weeks).
Rehabilitation can start the day after surgery during hospitalization and is continued in a centre or at the patient’s home with the assistance of a physiotherapist over a period of 3 to 6 months according to the type of arthroscopic procedures performed and to the patient’s recovery time. The first goal in rehabilitation being to restore a flexible shoulder.
The mean duration of hospitalization is from 2 to 3 days and variable according to each case. Some procedures can be planned at the ambulatory surgery unit.
Recent breakthroughs :
Resorbable suture anchors have been used for years and allow to avoid placing voluminous metallic materials while keeping a satisfactory and identical fixation to the bone. These anchors cannot be visualized by X-rays and scans. They allow to perform an MRI without interferences.
The addition to the tendon – bone junction, of biological factors facilitating tendinous healing during arthroscopic repair has been under assessment for a few years now. The objective is to improve the tendon repair quality and thereby reduce retear rates.





 Make an appointment
Make an appointment